On Friday, I was sitting at Solly’s final occupational therapy appointment of the week and I witnessed something amazing and entirely unexpected. Roughly two minutes after I hit publish on my last blog post, I looked up from my computer to see Solly, who was laying on his tummy, push his booty back over his knees and rise up into a quadruped position. This is a milestone that he’d never, ever achieved before, and here he was, exactly 8 weeks after an incredibly invasive surgery, placing a check mark next to a brand new milestone. I grabbed my camera and caught him in action for his next round, and here’s what I saw:
What a warrior!
It’s my hope that this milestone will help move Solly forward to more independence – more independent play, the ability to better interact with his environment, and perhaps even more gross motor milestones. Whether or not this is the case, we will continue to advocate to make all environments as accessible and inclusive as possible for Solly and his peers. In the meantime, we’re gonna celebrate the heck out of this major milestone!
Here are some other photos of Solly working so hard this past week:
I’ll continue to post progress updates on his rehabilitation here and on Instagram. Thank you to all for your kind words, thoughts, and prayers as Solly went through this surgery and for continuing to follow our journey.
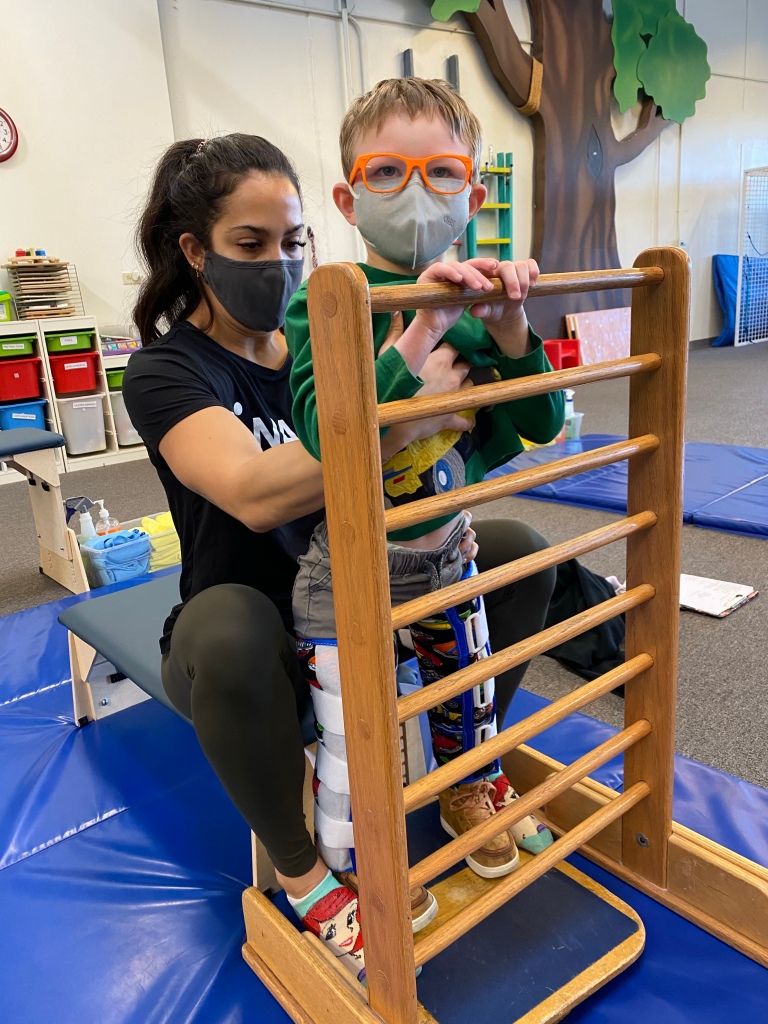
Oh, hi there! We have officially ended the first phase of recovery after Solly’s hip surgery. WOO HOO! On December 22, we had our second post-operative appointment with Solly’s medical team, and his X-rays looked perfect. We got the green light to start weight-bearing – and head back to physical therapy – with zero restrictions. It was such a relief and the best early Christmas present! The timing worked out perfectly for Solly to do a two week mini intensive at NAPA Center while their team was in between regular intensives, and the extra therapy has done wonders for Solly’s strength and confidence. He’s already back to army crawling, getting into an assisted four-point position, rolling with minimal assistance, and working so hard on standing on his new legs. At home, he’s been spending some time in his stander, going for daily bike rides, and doing short stints in his Trexo.
But, before I leave hip surgery in the past and start to focus too much on Solly’s rehabilitation, I wanted to touch on some of items that helped him recover at home immediately after surgery. In our experience, one of the most surprising parts in preparing for Solly’s hip surgery was the lack of at-home equipment suggestions the medical team provided for post-surgery. As a planner, this drove me bananas. I had no clue how we were supposed to support Solly overnight, where he would be spending his time during the day, or how transportation would look. I was even contemplating renting a wheelchair-accessible minivan to ensure we’d have enough room to accommodate Solly wearing a pillow wedge and leg immobilizers in a car seat. Fortunately, several Mamas answered my calls of distress when I took to social media to express my frustration and worries and provided suggestions of equipment to have on-hand, based on their own experiences. Here are the items that were the most helpful to us:
Social media can be a blessing and a curse. On one hand, since we received Solly’s diagnosis, I’ve been able to connect with, learn from, and befriend so many Mamas who are walking a similar path as mine. Their insights and guidance have helped me to navigate so many tricky situations. On the other, the groups where I’ve met these mothers can quickly turn into a rabbit hole when your child receives a new diagnosis or medical recommendation. You hear the good, the bad, and the ugly, with the bad and the ugly often standing out significantly, especially when it comes to surgeries.
That’s why, when we received the recommendation for Solly to have the VDRO and pelvic osteotomy surgeries, I was in despair. I kept reading horror stories of extreme discomfort, muscle spasms, and endless pain that goes on for months and months. These surgeries are painted in the worst light, making it truly terrifying to even consider your child going through them.
What’s important to know is that the doctor, medical team, procedures for pain and bracing afterwards, and the child’s medical history all play an important role in how this surgery can play out. Every child’s experience can and will be different.
Three weeks ago, Solly had a bilateral VDRO and pelvic osteotomy. It was a tough and long surgery. The immediate recovery while in the hospital was equally tough. He’s lost a bit of strength and we dealt with pain, muscle spasms, and some nasty side effects of pain medications. We still don’t know what’s to come in another three weeks when he’s able to start weight bearing and rebuilding strength. I suspect it’ll take months for Solly to physically get back to where he was pre-surgery.
Buzz helping Solly in the recovery room
But, despite what I’d envisioned – a recovery full of pain and agony, Solly is happy. He’s comfortable. And we made it through surgery.
Fortunately, we don’t have stories of Solly being in continual, unbearable pain. In fact, aside from some initial pain and some GI issues related to pain medications and immobility, much of his recovery has been manageable. Not easy, but manageable. I know this is not everyone’s experience and I also know that when you’re faced with the prospect of this surgery, you want to do all the research and go into the decision fully informed. Keeping that in mind, I wanted to share a bit of our experience with the surgery and recovery to give more insight – and maybe some hope – for families who need to consider this surgery.
I hate writing this. I hate saying this. I hate even thinking about this.
The “this” I’m referring to is Solly’s upcoming hip surgery.
I’m almost in tears even writing these words, though I’ve known it was coming for many months now.
Solly is having bilateral Varus Derotational Osteotomy (VDRO) and a left-side Pelvic Osteotomy surgery in mid-November.
And I’m having trouble coming to terms with it. Or, maybe more appropriately, I’m having huge amounts of anxiety over it.
This is the highly invasive surgery that we did everything in our power to postpone or avoid altogether by undergoing SPML when Solly was 2 and a half and later SDR and adductor lengthening surgeries when he was 5. We knew it was a likely event, but like everything else when parenting a child with a disability, we hoped and prayed that he would be the one exception that could avoid it.
That wish turned out to be a big fat “nope”.
The background: Why do kids with cerebral palsy often face this surgery?
In short, Solly needs to have this surgery because he has hip dysplasia. His hip sockets are super shallow and the head of his femur, or thigh bone, doesn’t fit properly inside his hip sockets. His right leg is about 30% out of the socket and his left is over 50% out.
Oftentimes, when kids have diplegic (involving both legs), triplegic (in particular, those involving two legs and an arm), or quadraplegic (involving all four limbs) cerebral palsy, the tight muscles of the legs pull the legs out of the hip socket. For Solly, this started occurring when he was around 2 years old, but SPML plus alcohol blocks, which relaxed his legs, allowed for his hips to go back in the socket. Once the alcohol blocks from that procedure began to wear off, his hips began to slowly sublux again. Solly had SDR once we understood that his hips were beginning to dislocate again, however because his cerebral palsy is spastic and dystonic, and SDR only solves for spasticity, this only slowed the dislocation. It was not an effective solution.
Some doctors will do a lower body cast after the surgery to protect the hips, however we opted to go with a doctor who provides removable leg braces and an adductor pillow wedge post-surgery. Solly will wear these for about 6 weeks after surgery and will not be able to bear weight for that amount of time.
Will the surgery help Solly?
Yes. The first orthopedic surgeon in Los Angeles who told us we needed to consider surgery said the procedure was primarily to minimize pain, particularly as Solly grew. However, as I read through that particular doctor’s clinical notes I realized that he did not listen to my accounts of Solly’s progress and ability and noted that he had not made any progress throughout the prior year and, for example, only walks in a gait trainer while at therapy. His plan was to just do the bilateral VDRO and place Solly’s hips at a severe angle to keep them from dislocating again and requiring repeat surgeries. The “severe angle” piece did not sit well with me and I read his plan as an action that could hinder Solly’s physical development. Those notes prompted me to seek out a second opinion, particularly at the suggestion of an adult with cerebral palsy who went through this surgery twice.
According to the doctor who gave us our second opinion and who is the doctor that will perform the surgery, the combination of VDRO and pelvic osteotomy will not only help minimize any hip pain as Solly gets older, but the addition of the pelvic osteotomy should help stabilize his pelvis so that he can walk without scissoring and hopefully get stronger in all of his ground and weight-bearing abilities. As with all things related to cerebral palsy, we remain realistic that this surgery will minimize any joint pain he might have as he grows up and are hopeful that it will help our goals of allowing Solly to become as independent as possible.
So, what’s next?
Solly has to get a number of sign offs in order to proceed with the surgery, most notably from a hematologist. Our worry with an orthopedic surgery that requires six weeks of immobility is the formation of blood clots, particularly since Solly is a stroke survivor and has several blood clotting disorders. We’re hopeful that the hematologist will sign off on the surgery and provide guidance so we can mitigate any risks associated with blood clots.
Once this happens, we’ll go through the surgery in mid-November and plan to celebrate by removing the leg immobilizers and adductor wedge on Christmas Eve, which is exactly 6 weeks post-surgery. I’m planning to take Solly to his weekly speech and occupational therapy appointments starting about 10 days after surgery rather than break from all therapy. Solly’s NAPA Center therapists are his favorite people and wheeling into the clinic, for Solly, is like going into “Cheers!” – we simply couldn’t keep him away for 6 whole weeks! However, he will be taking about 6 weeks off from physical therapy and will start up again at least once per week as soon as we get the “ok” from his surgeon. We’ve already set up intensive therapy at NAPA for February 2022 so we can hit the ground running and start working on building up his strength post-surgery.
As I indicated when I started this post, the news of this surgery is devastating to us. This surgery is known as one of the tougher surgeries in the CP world and one that is particularly painful and rather difficult to bounce back after. I try to remain positive, but it’s really hard to not imagine the worst-case scenario. I think, as parents of a disabled child, whenever something is going well, we’re all consciously – or subconsciously – waiting for the other shoe to drop. So, with that, I’ll close out with a promise to either post an update or two here on Solly’s blog or on my Instagram account as we go through the surgery and recovery.
The other day, a video popped up on my Facebook memories. It was from a year ago, capturing the first time Solly said, “no!” It may not seem like much, but we were so thrilled that, at age 5, he was finally (finally!!!!!) saying “no” appropriately and unprompted.
This video was taken roughly a month and a half before we began our trial with medical cannabis. Since then, Solly has been communicating – both speaking and using augmentative and alternative communication (AAC) – so much that it seems hard for us to remember the time when we ached for him to be able to tell us what he was thinking or what he wants, so when these memories pop up on social media, it helps us to recognize how far he has come in such a short time. While he had a handful of words before medical cannabis, we still struggled to really understand his preferences, what he wanted to do, and what he wanted to eat.
In mid-March of 2020, we had our first appointment with Dr. Bonni Goldstein, which kickstarted our trial with cannabis. I wrote a bit about our experience with CBD and THCa a few months later, when we first saw an unbelievable explosion of expressive speech. Shortly after writing the blog post, keeping up with our experimentation flew off my plate as I became hyper-focused on Solly trying to get an IEP before the start of school, deciding to pull him from public school, feeling like I was thrown in the deep end of the pool without knowing how to swim as I navigated putting together and teaching a homeschooling curriculum while being the primary caregiver, home therapist, medical coordinator, Mom to both Solly and Bea, and so much more.
Once I got my feet back under me and got into the groove of homeschooling and more organized with our day-to-day, we jumped back into our trial-and-error adventure with medical cannabis.